The University Hospital Center of the Algarve (CHUA) has the only reference center recognized by the Ministry of Health in the Algarve and Baixo Alentejo. It is the Rectal Cancer Reference Center.
South of the Tagus, there are only two more Reference Centers for other pathologies, one at the Garcia de Orta hospital, in Almada, and the other at the Espírito Santo Hospital, in Évora.
This Algarve Centre, which was created in 2016 and completed its certification and accreditation process by the General Directorate of Health in 2018, is currently treating around 400 patients from across the Algarve region. Dr. Edgar Amorim, a specialist in General Surgery and coordinator of the Reference Center, told the Sul Informação that the average number of new patients arriving per year is a hundred. But as its treatment takes, on average, five years, there are now about four hundred to be followed.
But what is a Reference Center and what is it for? Edgar Amorim explains that «the creation of the reference centers was a bet of the Ministry of Health in 2015. Basically, what they did was to pick up certain pathologies that, due to their specificity or their need for resources, had to be concentrated in certain teams, as a way to achieve the best results, both clinical and economic».
Thus, «the conditions were created so that these pathologies can be concentrated in highly differentiated teams, trained to achieve good results».
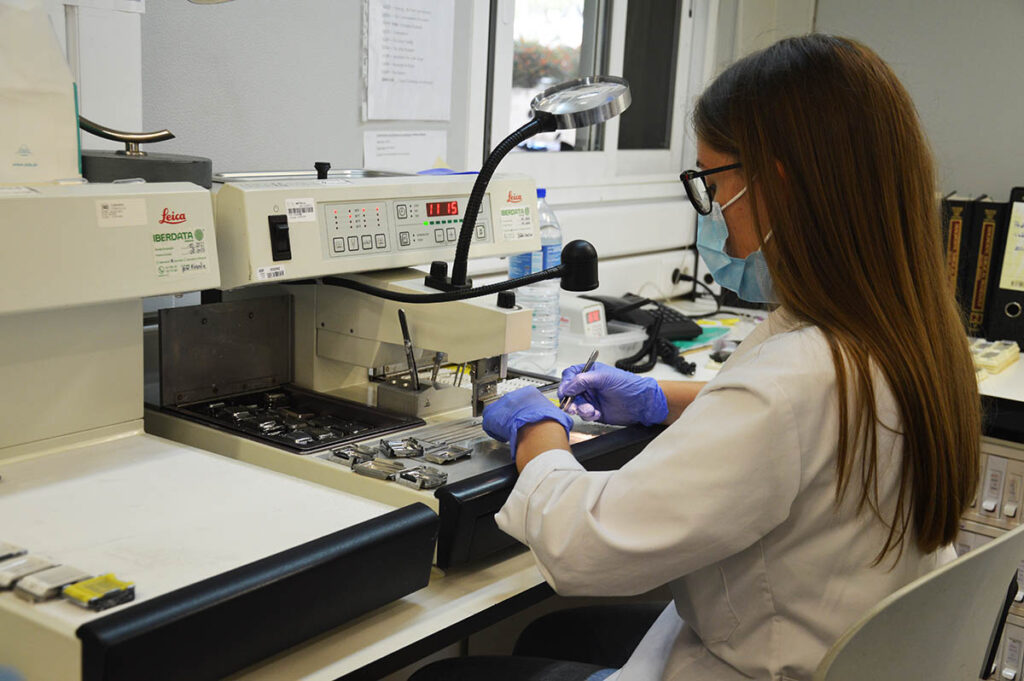
The official adds that “CHUA's Rectal Cancer Reference Center is formed by a multidisciplinary team, involving doctors, nurses, nutritionist, therapists and managers, also having a strong multidisciplinary component. Clinicians from different specialties are involved, namely pathological anatomy, general surgery, gastroenterology, medical oncology, radiology and radioncology, who jointly ensure the treatment of patients, based on high technical standards».
"Having a reference center at CHUA is having a guarantee that patients in the Algarve are treated with the best standards, the best techniques and the best quality, which is at the level of any center that treats this type of pathology in Europe", he assures the one responsible.
An added value is the fact that, as it exists within CHUA, this Reference Center is linked to the University of Algarve. «One of our goals is research and research in the Algarve. Our reference center has all the conditions to develop research processes, not least because it is directly associated with the academy», explains Edgar Amorim.

In the Algarve region, the prevalence of rectal cancer among the population is similar to that of the rest of the country, with the average age of people with this pathology being 67 years. If this is not a more serious problem in the region than in the rest of the country, why create this Reference Center here?
Paulo Caldeira, director of the CHUA Gastroenterology service and also a member of the coordination team of the Reference Center, explains that it was an «application process», considering «the know-how, the experience, people and technologies" that already existed in the two main hospitals in the Algarve, those of Faro and from Portimão. Basically, the creation of these reference centers forced "services, hospitals, to provide more differentiated and more excellent care, in some pathologies that are rarer, more difficult or complex to treat".
Both these two doctors and the nurse José Brás, who is also part of the core of the coordination team of the Reference Center, emphasize that, in this cancer, as in all others, it is important that patients are diagnosed as soon as possible. With the difference that, in rectal cancer, if the diagnosis is made at an early stage, there is now an 80 to 90% chance of survival after five years, in other words, in simpler terms, of survival.
That is why, they insist, screening is so important. This is a task that is not even part of the work of the Reference Center, since, in recent years, it was the Regional Health Administrations that started to promote regular screening for cancer of the rectum. And both in these regular campaigns, as in fortuitous appointments with the family doctor, many patients are caught in the early stages of the disease, that is, in a more treatable stage.
But the pandemic changed this state of affairs. “This last year was a little atypical, because there was a reduction of about 25% of the patients who come to us”, laments Edgar Amorim. Furthermore, “patients are reaching us at much more advanced stages”.
That's why, in an initiative that the Sul Informação has been supporting, the Reference Center has started to promote the need for people to be screened by publishing in our journal, articles by various experts to demystify and clarify.
People who already have symptoms, such as blood in the stool or changes in intestinal transit, should be screened as soon as possible. «Nowadays, the ideal was to be able to diagnose these injuries at a stage where they have practically no symptoms. And there are simple ways to do this, by searching for occult blood in feces and then, if necessary, performing a colonoscopy, in which polyps or very early cancers can be detected», adds Paulo Caldeira.
"In an ideal world, from the age of 50, everyone should have a form of screening, in order to detect lesions as early as possible, because the treatment, that is, our treatment possibilities and the probability of success are today completely different», says the director of Gastroenterology at CHUA.
But many of the cases are detected through what is called "opportunistic screening", when "people go to the family doctor and he remembers to tell them to do a fecal occult blood test and, if positive, do one colonoscopy".
“The problem is that not all people are covered by screening, because there is no summons system”, stresses Paulo Caldeira. The summons system, similar to breast cancer screening, he recalls, started a little over two years ago, but the pandemic made the process stop and even regress. Therein lies the explanation for the drop in a quarter of new rectal cancer patients arriving at the CHUA Reference Center: fewer diagnoses and more difficulty in accessing the NHS result in fewer patients being detected.

One of the great resistances of people to being screened for this type of cancer is the fear of colonoscopy. Nurse José Brás admits that “there is still a myth surrounding colonoscopy”.
“In the past, it was done with worse devices, with less experienced people, and exams could sometimes be a little painful and unpleasant experience”, he admits. But “it's not like that anymore: the devices are much better, easier to handle, we have many more technicians and more experienced and, above all, we have, in most situations, the support of the anesthesiologist. The exam is painless, it doesn't cost much. The preparations that have to be made are already better tolerated”, he guarantees.
Returning to the question of screenings. When these were more systematic, patients were caught 'at an earlier stage'.
But that changed, with the constraints brought by the pandemic. What are the consequences of this? “In terms of patient survival, it is expected that these patients will survive less, there will be a decrease in survival or in their ability to be alive after 5 years”, admits Edgar Amorim.
"These patients will have to undergo much more aggressive treatments, which may involve chemotherapy, liver surgery, therefore procedures much more aggressive and invasive," he explains. And, even from an economic perspective, “we are talking about much higher costs to guarantee the treatment of these patients who come to us at more advanced stages. We will have to use more human, diagnostic, therapeutic means, more means at a higher cost, because we have not managed to do the disease prevention part», laments the coordinator of the Reference Center.
But neither Edgar Amorim nor the entire team lower their arms, quite the opposite. “It is important to be aware that the treatment of oncological diseases, and in particular cancer of the rectum, has evolved a lot in recent years. About 40 years ago, the survival rate was 30 to 40%. And right now we have survival rates of 80 to 90%».
So what should people expect from the Reference Center? The coordinator guarantees that here the patients (and their families or support network) will be “evaluated and guided by multidisciplinary teams, which will make the diagnosis and correct staging of these lesions”.

The first reception of the patient, either in the hospital unit of Faro, either in Portimão, is carried out by the nursing team that integrates the Reference Center.
In the capital of the Algarve, nurse Isabel Botelho explains what is done: «we are the ones we caught the sick as soon as he arrives. We give the good or bad news and follow it from here, until the end of the process. Go to surgery and back, go to radiotherapy and back. The nurse who receives you here at first is usually the one who accompanies you until the end of the process».
These nurses end up being the “point of reference” for the patient, who thus does not feel lost. “Because afterwards, radiotherapy is with a doctor, surgery is with another and so on. But the nurse who catch the patient here, from the beginning, is always the same».
Nurse Daniela Costa, at the hospital in Portimão, adds that, when the patient arrives there, “they already come with many fears and fears, they have already researched in the doctor Google, comes with pre-made ideas and this consultation and nursing explains the entire process that will happen to him from that moment and clarifies all the doubts and fears with which he arrived at this consultation». And this explanation is given "both to him and to the relatives who accompany him". And it remains available throughout the entire process.
Basically, he stresses, “we are the face”, which humanizes an always frightening process.
Doctor Edgar Amorim adds that the nursing team «has another important role here, which is, in addition to the social assessment of the person, to know what can be expected from the family».
The nursing team that integrates the Reference Center is coordinated by the nurse Ricardo Mestre, who is part of the «nuclear team». "We have always participated in what is asked of us and contributed to make things work within what is recommended, in order to provide care more adjusted to the needs of our patients," he guarantees.

Another important element in the Reference Center team is the nutritionist. “These patients often come to us with nutritional deficits and are immediately referred to the nutrition consultation on the same day, if necessary. They are patients with vitamin deficiencies or chronic anemia», explains Edgar Amorim.
Radiology is also a key element of the Reference Center, which is fundamental for diagnosis and staging, by CT or Magnetic Resonance. “Radiology is a fundamental service, because a staging that is not as accurate as possible can lead to decisions that are not the most adequate”.
The specialist physician Jorge de Brito, from the Faro, is responsible for this work at the Reference Center. "My subspecialty area is abdominal radiology," he explained to Sul Informação, which means that, «at the Reference Center, the exams that are carried out on patients with rectal cancer are not carried out by any radiologist».
The "temporal window" in which examinations are carried out is "fundamental". There is, in fact, no waiting list for rectal cancer patients. «The big problem is that the Radiology service does not only respond to the Reference Center. This requires an organization so that we can give a positive response, both in terms of time, reducing patient waiting times as much as possible, and in terms of quality, there it is, because these exams cannot be done by anyone».
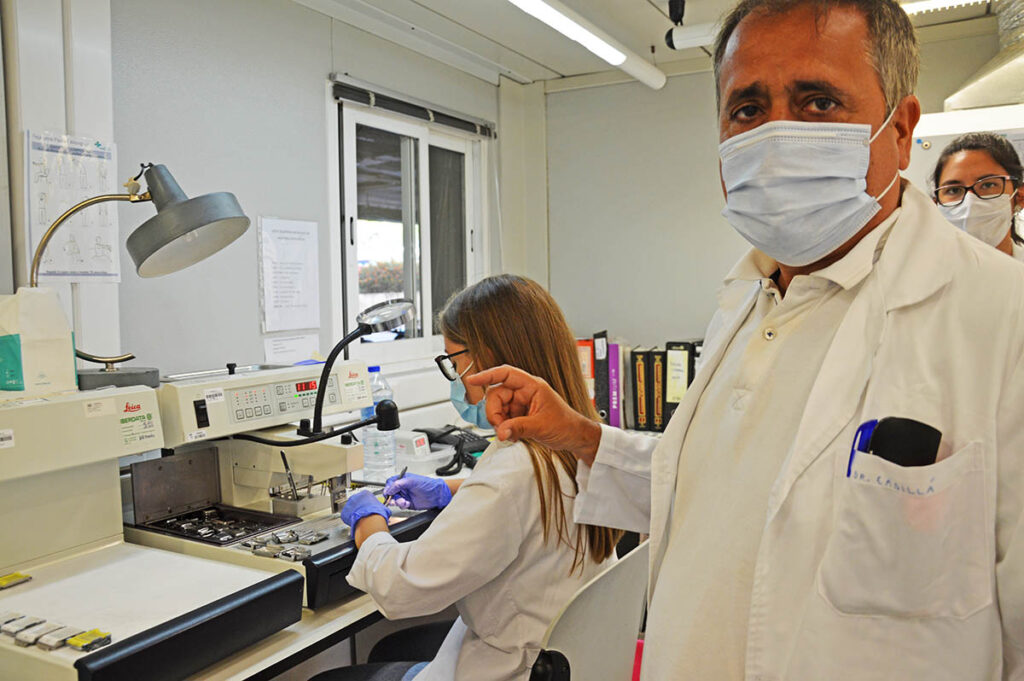
The Pathological Anatomy, installed in Faro, is another key service. Its responsible is the specialist doctor Jesus Cadillá, who, according to coordinator Edgar Amorim, heads a service that works “almost like our police officers”.
In this multidisciplinary team there is also Oncology. Nor could it be otherwise since it is cancer that is talked about. The report of Sul Informação he went to meet the specialist doctor Pedro Santos at the Oncology Day Hospital, at the Portimão hospital unit.
In relation to cancer of the rectum, oncologist Pedro Santos guarantees that, «contrary to what many people think, the genetic component is relatively small in relation to this type of neoplasia». What explains the appearance of this disease is the "predominance of bad eating habits", since "sugar is terrible, red meat too", but also the "sedentary lifestyle, obesity".
Therefore, he argues, “we must always bet on screening and early assessment. Because there is a difference between being able to cure an aggressive disease, but at an earlier stage, or an incurable disease».
“This is a good bet for Dr. Edgar, who is the mentor of the Reference Center. It is a highly specialized and differentiated center that allows the correct treatment of patients. I think the Algarve deserves it and it has a good surgical team, it has a good oncology team. This partnership between all comes to help in that aspect», stressed, in conclusion, Pedro Santos.

Working with a multidisciplinary team makes all the difference. Because, thanks to this approach, each patient is not given a «treatment standard» The same for everyone, stresses coordinator Edgar Amorim. On the contrary.
"Although today we have a lot of technology and we have access to different drugs that we didn't have a few years ago, for me the great evolution in the treatment of oncological disease is the multidisciplinary assessment, focused on that specific patient and that takes quality into account of your future life. That image that we often had, that the patient was undergoing treatment standardized, that nowadays no longer exists. We use to say “the cancer that the neighbor has is a different cancer than the one this patient has”. There is now a personalized, multidisciplinary decision that takes into account the patient's future quality of life. In other words, we assess the individual with the disease and not just the disease itself».
One of the situations that Edgar Amorim considers that it is necessary to “demystify” is that “fast is not always good”, not even in cancer. “Going fast sometimes isn't important. It's important to do well. To stay is to understand exactly all the involvement of the tumor and then, from there, make the best treatment decisions, by the team, by the various professionals. Because afterwards this always involves a long treatment and almost always involves a previous chemotherapy and radiotherapy treatment. This is one of the great changes of the last 20 years: you don't operate straight away, first you have chemotherapy or radiotherapy, which takes several weeks, and then, if it's still necessary, surgery».
The specialist doctor Pedro Santos had already explained this: «oncology, together with radioncology, have a very important role in these types of treatments», because they manage to act «on tumors that may not have an indication for surgery or whose surgery may be very difficult». “Chemotherapy and radiotherapy, when applied before surgery, are able to regress or reduce the size of the tumor, in order to be able to perform surgeries that were not possible in the beginning. And, in some cases, they even manage to completely eliminate the tumor», without having to resort to surgery.

The article goes on for a long time, but there is still a need to address a topic that scares many people, when it comes to cancer that affects the intestines, whether in the colon or rectum: the colostomy, that is, the sac where feces come out.
“Definite colostomy is becoming less frequent. There are new techniques», guarantees the nurse José Brás.
“Even in that regard, things have evolved a lot. If, a few years ago, there was a high probability that patients would stay with the colostomy for life, nowadays these indications are starting to be increasingly reduced», he adds.
But it is a fact that many patients will depend on the colostomy bag. However, in addition to, at the moment, the devices are much easier to use and replace, this aspect is not forgotten by the Reference Center. «There are own consultations, both in Faro as in Portimão, where people who are already in the final stage of their treatment or who are going to live their entire lives are monitored” with the colostomy bag.
“This concern frightens us, when we don't know it, when there are many myths, which is why it is necessary to clarify. I remember a young woman who has one of those bags through which feces come out and who, after her surgery and after the bag was placed, decided, together with her husband, to become pregnant and have their child. In other words, when you think "there's going to be a bag and it's going to be terrible", it's actually a problem at that moment, but let's live with that issue and make it stop being a problem, to become a life situation », says José Brás. The nursing team that closely monitors each patient who enters the Reference Center is, once again, “fundamental”.
Surgeon Edgar Amorim corroborates: «today, having a colostomy does not necessarily mean that the person does not have quality of life. There are people with colostomies who do marathons. There are people with colostomies who go about their normal life, who get pregnant, can swim. Hence, also, the importance of having, in the Reference Center, teams prepared to deal with these situations».
All patients with rectal cancer are discussed weekly by the core team in a multidisciplinary group meeting. This “enables us to guarantee that our patients have a therapeutic option validated according to best practices. Currently, the therapeutic options at our center differ only occasionally from the offers that may be offered by other national or international centers. This is certainly an asset for our population, knowing that in their area of residence they can access the best treatments available today», stresses the coordinator of the only Reference Center in the Algarve and Baixo Alentejo. Moreover, he says, rectal cancer, "in terms of the digestive tract, it is the most frequent, but it is also the most treatable".
For more because, as he makes a point of emphasizing, at CHUA, both in the unit of Faro, as in Portimão, «there are no limits of places for rectal cancers. In other words, the limit number in the first consultations of this week is the number of orders that arrive to us. According to the latest official and published data, we had a response time of approximately 9 days, which places our center well below the times defined by law and demonstrates the ability of the Reference Center to respond to these requests. There is no waiting time, no list». And that alone is good news.

Colorectal cancer situation in Portugal and the Algarve
Colorectal cancer has become an important indicator of international public health, and its results and instituted policies are being monitored by different national and international organizations.
Known 2020 data reveal that, in Portugal, there were 10500 new cases of colorectal cancer, corresponding to about 17% of all new cancers diagnosed. Colorectal cancer, when evaluated together by both sexes, occupies the 1st position in the ranking of new cases per year. Alone, rectal cancer was responsible for about 8,2% of new cases, approximately about 5000 cases.
Of the 30.118 deaths that occurred in 2020 in Portugal due to cancer, 4320 (14,3%) were due to this type of cancer, which places it as the 2nd cause of death due to cancer.
However, it is not all bad news, as the death rate has been gradually declining. For example, in the Algarve, official data for 2018 and compared to 2015 show a decrease in deaths from colon cancer of around 34% and around 10% in rectal cancer.
Up until the mid-80s, rectal cancer had a survival rate after 5 years of diagnosis of about 27 to 42%, which contrasts with the current 70 to 80%. The recurrence rate also increased in the same period from 30% to 8%.
For this to be possible, the great effort that the health institutions and, in particular the CHUA unit, has made in the creation of highly differentiated teams and in the implementation of screening programs has contributed a great deal.
What is colorectal cancer and how does it appear?
The digestive tract is formed by the set of anatomical structures that go from the mouth to the anus. It is along the digestive tract that food moves and undergoes transformation through a process called digestion, so that it can be absorbed. The colon (large intestine) and rectum are located at the end of the digestive tract.
Colorectal cancer develops due to the uncontrolled production of its inner lining cells. This process is usually slow and can take several years before there are symptoms that can alert you to its onset.
Initially, this uncontrolled production gives rise to benign tumors, known as polyps, which, when left untreated, can acquire different characteristics and transform into malignant tumors (Cancer).
In 85% of cases, there is no genetic or familial relationship with the onset of cancer. On the other hand, its association with certain eating habits is known, in particular the consumption of red meat and animal fat, with a sedentary lifestyle and the consumption of alcohol and tobacco.

What are the symptoms / warning signs?
Although there is no symptom that is unique to colorectal cancer, there are some signs that should sound the alarm and lead to an assessment in primary care, especially for those over 50 years old. It should be remembered that 90% of new cases happen over 50 years of age.
These alarm signals, when not looked for, can go unnoticed. They include the existence of alterations in the intestinal transit and its characteristics, the existence of blood in the stool, weight loss for no apparent reason, anemia.
Importance of Screening (patients without symptoms)
In Portugal and in accordance with the national plan for the prevention and control of oncological diseases, screening for colon and rectal cancer in asymptomatic individuals, that is, without any symptoms, must be carried out between 50 and 75 years of age.
The recommended method is the investigation of fecal occult blood, a non-invasive test. If it is positive, it is later advised to perform a colonoscopy.
Regular screening can prevent the disease, as colon and rectal cancer grow slowly from the onset of the precursor lesion to its transformation into cancer.
The reduction in mortality and the increase in survival is directly related to the stage of the disease (stage) in which it presents itself. Thus, the earlier the diagnosis, the greater the probability of successfully overcoming this stage of life.
Photos: Elisabete Rodrigues | Sul Informação (except for surgery images)
























Comments